
Lysinuric Protein Intolerance
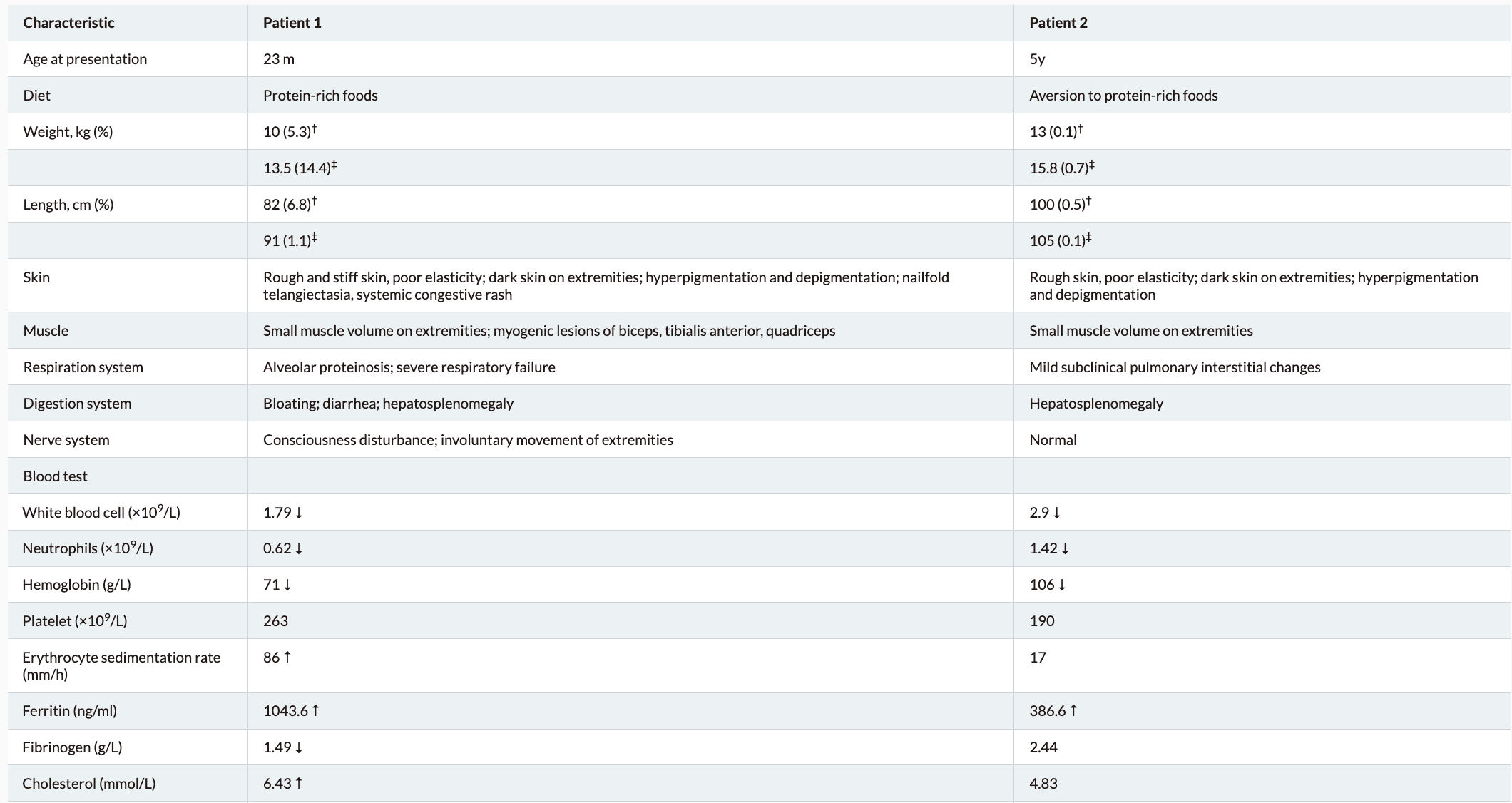
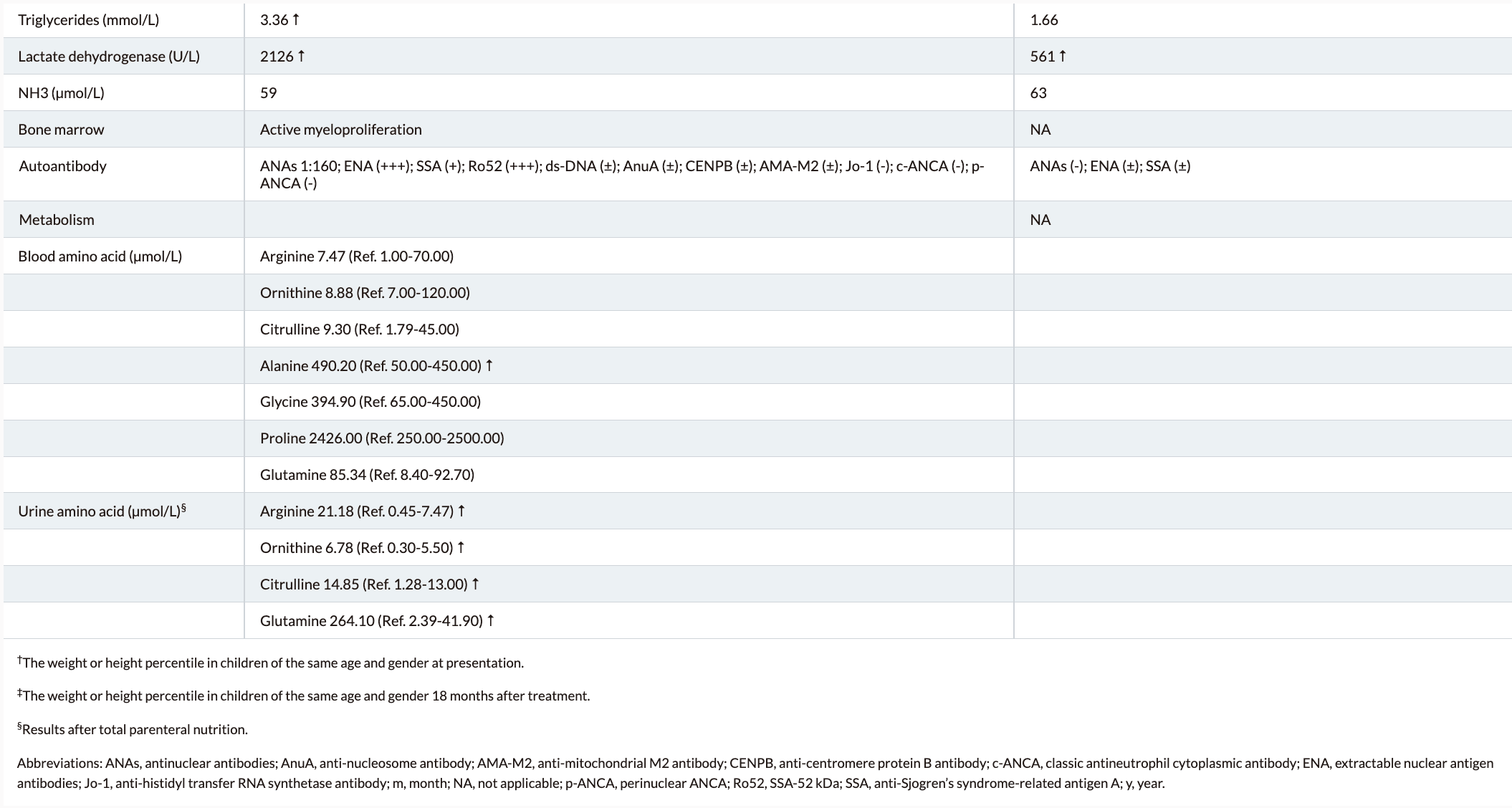
Lysinuric protein intolerance (LPI) is a rare autosomal recessive disorder caused by mutations in the solute carrier family 7A member 7 (SLC7A7) gene.1 It is characterized by protein intolerance, secondary urea cycle disorders, and immune dysfunction after consuming protein-rich food in the post-weaning period.2 Here, we report two siblings from a family with LPI who share the same genetic phenotype and exhibit similar clinical manifestations. However, the severity of their symptoms varies greatly due to differences in dietary intake.
Clinical presentations and symptoms of Lysinuric protein intolerance (LPI)
Lysinuric protein intolerance (LPI) typically presents after an infant is weaned from breast milk or formula; variable findings include recurrent vomiting and episodes of diarrhea, episodes of stupor and coma after a protein-rich meal, poor feeding, aversion to protein-rich food, failure to thrive, hepatosplenomegaly, and muscular hypotonia. Over time, findings include: poor growth, osteoporosis, involvement of the lungs (progressive interstitial changes, pulmonary alveolar proteinosis) and of the kidneys (progressive glomerular and proximal tubular disease), hematologic abnormalities (normochromic or hypochromic anemia, leukopenia, thrombocytopenia, erythroblastophagocytosis in the bone marrow aspirate), and a clinical presentation resembling the hemophagocytic lymphohistiocytosis/macrophagic activation syndrome. Hypercholesterolemia, hypertriglyceridemia, and acute pancreatitis can also be seen.
LPI is a congenital genetic metabolic disease with multisystem involvement. Initiating appropriate protein-restricted diet therapy as soon as possible could help prevent the progression of LPI.
How Is It Managed or Treated?
Treatment of manifestations: In acute hyperammonemic crises: intravenous administration of arginine chloride and nitrogen-scavenger drugs (sodium benzoate, sodium phenylacetate) to block ammonia production; reduction of excess nitrogen in the diet; provision of energy as carbohydrates to reduce catabolism. Long-term: dietary protein restriction; oral supplementation with citrulline and nitrogen-scavenger drugs, L-lysine-HCl, and carnitine; whole-lung lavage to improve respiratory function in persons with pulmonary alveolar proteinosis.
Prevention of primary manifestations: Long-term protein restriction and administration of citrulline and nitrogen-scavenging drugs.
Prevention of secondary complications: Minimize the risk of respiratory infections; vaccination against influenza is recommended. Varicella immunization in those without previous history of chickenpox or varicella zoster; treatment of those exposed as immune-compromised persons; revaccination may be required if poor response to polysaccharide-containing vaccines.
Surveillance: Plasma concentration of amino acids to identify deficiencies of essential amino acids secondary to protein-restricted diet; fasting and postprandial blood ammonia concentrations and attention to signs of hyperammonemia, urinary orotic acid excretion; periodic evaluation of renal function; evaluation of lung involvement; periodic serum LDH and ferritin.
Agents/circumstances to avoid: Large boluses of protein or amino acids.
Evaluation of relatives at risk: It is appropriate to evaluate at-risk sibs of a proband by molecular genetic testing or biochemical testing in order to reduce morbidity and mortality through early diagnosis and treatment.